
Pancreatic cancer remains one of the most difficult malignancies to diagnose and treat, largely because early-stage disease is often asymptomatic. Despite decades of research, outcomes for patients with metastatic pancreatic ductal adenocarcinoma have remained poor, with limited treatment options available after first-line therapy fails. Current imaging modalities frequently fail to detect localized disease until tumors have progressed beyond the earliest stages, contributing to the persistently high mortality associated with this cancer. For decades, second-line treatment options have offered only modest clinical benefit, with median survival typically measured in months rather than years.
To understand why the ground fundamentally shifted this year in Chicago, one has to look back more than forty years to 1982, when the KRAS oncogene was first discovered and cloned. For four decades, the global research community understood the primary genetic engine driving many pancreatic cancers, yet remained unable to effectively inhibit it. The mutated protein’s smooth, globular structure lacked the accessible binding pockets required for conventional small-molecule drug design. It repeatedly defeated generations of targeted therapeutic approaches, earning a reputation as one of oncology’s most elusive targets. It required decades of advances in structural biology, medicinal chemistry, and translational science to finally bridge the gap between laboratory discovery and clinically effective therapy.
That historical frustration is precisely why this year’s ASCO 2026 plenary session became an immediate landmark moment. When the final survival curves from the Phase III RASolute-302 trial were presented inside a packed McCormick Place auditorium, the response was a spontaneous standing ovation from clinicians in attendance. The applause reflected more than the achievement of a statistically successful clinical endpoint; it represented a collective acknowledgment that medicine had finally overcome a four-decade challenge against one of cancer biology’s most formidable pathways.
The landmark trial evaluated Daraxonrasib, an oral, once-daily multi-selective RAS(ON) inhibitor developed by Revolution Medicines. For patients navigating the harsh landscape of previously treated metastatic pancreatic cancer, the definitive data presented by Dr. Brian M. Wolpin of Dana-Farber Cancer Institute positions Daraxonrasib to become the new standard of care in the second-line setting, shattering the historical survival ceiling that has constrained secondary systemic therapy for decades.
The clinical prognosis for metastatic pancreatic adenocarcinoma remains one of the most formidable challenges in modern medicine, with approximately three percent of patients surviving five years after diagnosis when distant metastases are present. Once frontline chemotherapy regimens inevitably fail because of disease progression or treatment resistance, secondary options have historically provided limited therapeutic benefit. The RASolute-302 trial challenged these longstanding expectations by enrolling 500 patients globally who had progressed on exactly one prior systemic therapy and randomizing them to receive either oral daraxonrasib or investigator-selected standard chemotherapy.
The resulting data met its dual primary endpoints with a remarkable separation between the survival curves. Daraxonrasib delivered a 60% reduction in the risk of death, reflected by a hazard ratio of 0.40. In a historic milestone for targeted monotherapy in this setting, median overall survival increased to 13.2 months in the daraxonrasib arm compared with 6.7 months in the chemotherapy cohort. Progression-free survival similarly improved to 7.2 months compared with 3.6 months in the control arm, while objective response rates reached 31.6%. Importantly, while the trial primarily focused on patients with RAS-mutated disease, the observed clinical benefit extended across a broad range of RAS alterations.
The reason daraxonrasib succeeded where previous approaches struggled lies in a fundamentally different structural strategy. Rather than attempting to bind a difficult target directly, the therapy employs a tri-complex mechanism involving cyclophilin A, a naturally occurring intracellular protein. The resulting molecular complex creates a new interface capable of binding and suppressing the active, GTP-bound state of multiple RAS variants simultaneously (Fig.1). By effectively using the cell’s own biology as a molecular scaffold, daraxonrasib inhibits signaling across multiple oncogenic RAS alterations, overcoming the variant heterogeneity that limited earlier targeted approaches.
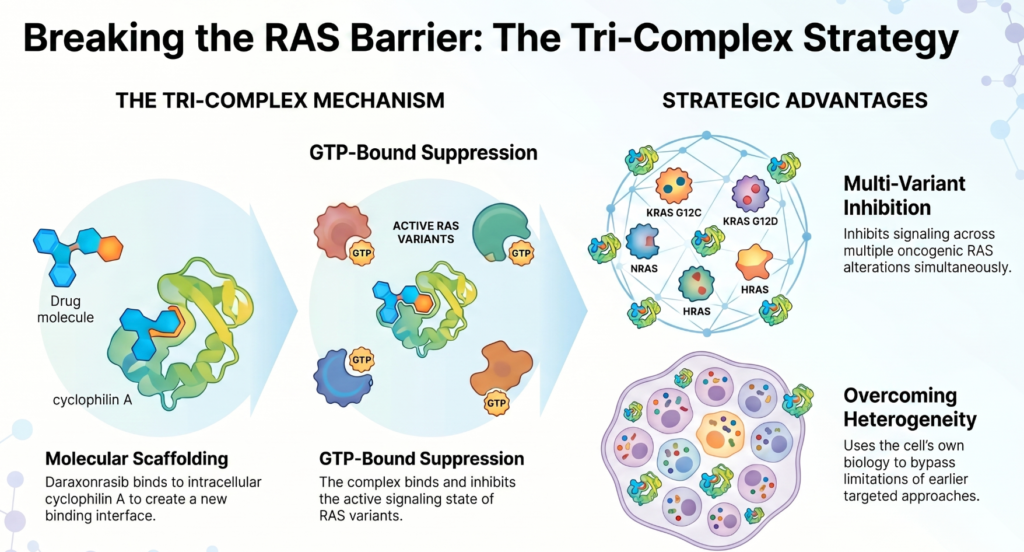
Fig.1 AI Generated Image
From a clinical operations and patient-care perspective, the significance of RASolute-302 extends beyond survival metrics. Traditional salvage chemotherapy is associated with substantial toxicity, including severe neutropenia, thrombocytopenia, and peripheral neuropathy, all of which can significantly affect quality of life and treatment adherence. Daraxonrasib offers a fundamentally different treatment experience by transitioning patients from infusion-based therapy to a once-daily oral regimen administered at home.
The safety profile observed during the trial underscores this advantage. Treatment discontinuation due to adverse events occurred in only 1.2% of patients receiving daraxonrasib compared with 11.2% of those receiving chemotherapy. Severe treatment-related adverse events were also reduced. Investigators further reported meaningful clinical improvements among many patients during therapy, complementing the survival and response-rate findings and suggesting the potential for prolonged survival alongside preservation of functional independence and quality of life.
The momentum generated in Chicago has already accelerated activity throughout the oncology community. Expanded access efforts and regulatory review processes are underway to help make daraxonrasib available to eligible patients ahead of formal commercial approval. Simultaneously, the research landscape is rapidly expanding into earlier treatment settings. The ongoing Phase III RASolute-303 trial is evaluating Daraxonrasib in previously untreated metastatic pancreatic cancer, including both monotherapy and combination strategies alongside standard frontline chemotherapy regimens.
The central mission of modern clinical research is the translation of molecular science into meaningful patient outcomes. By transforming a highly complex and historically untouchable oncogenic pathway into a clinically actionable therapeutic target, the RASolute-302 trial delivers on that promise in extraordinary fashion. For clinicians, investigators, and trainees alike, it stands as a powerful example of translational medicine at its best demonstrating that even the most entrenched biological challenges can eventually yield to persistence, innovation, and scientific rigor.
For patients facing one of the deadliest malignancies in oncology, the significance is even more profound. The story of daraxonrasib is not simply one of a successful drug. It is the story of a forty-year scientific pursuit that has finally begun to translate into additional time, improved outcomes, and renewed hope for a population that has historically had far too little of all three.
References:
1. Wolpin, B. M., Park, W., Garrido-Laguna, I., Spira, A., Starodub, A., Sommerhalder, D., … & Hong, D. S. (2026). Daraxonrasib in previously treated advanced RAS-mutated pancreatic cancer. New England Journal of Medicine, 394(18), 1790-1802
2. https://www.nytimes.com/2026/05/12/health/pancreatic-cancer-daraxonrasib-kras.html
Leave a Reply